Nitrous Oxide and Its Use In Childbirth for Pain Relief
Most of the folks who come to my Confident Birthing Childbirth Classes are preparing for a natural childbirth. They hope to avoid the use of pain medications in their births. Those
not intending a drug-free birth, are usually hoping to delay the use of pain medications and that means that they would be delaying/avoiding systemic narcotics (administered through an I.V.) and/or the most common pain management used in childbirth, the regional anesthetic: epidural.
Avoiding those drugs is most often possible through non-pharmacological means like movement, touch, breathing, intention, and sounding, just to name a few. I have spent my 20+ year career helping women avoid or delay those medications through my classes and my doula services. And while it’s still possible for women, whose goal is an unmedicated birth, to achieve that through good preparation and good support, there is another option for pain management here in the Treasure Valley that is worth knowing about: Nitrous Oxide.
Used around the world for well over 100 years as a medical analgesia, Nitrous Oxide is most commonly thought of in the United States as the “laughing gas” used by dentists to help ease patient’s anxiety during dental procedures. Discovered in the late 1700’s, it was introduced to provide pain relief during childbirth in 1881 but its wide use increased in the 1930’s when an apparatus was developed for self-administration. Since that time, laboring women have been using nitrous with great satisfaction in Great Britain, Canada, Finland and Australia. However, in the United States nitrous fell out of favor in the 1970s and the US has been slow to implement this option for laboring women since.
In 2002, Childbirth Connection conducted a systematic review of the research on pain management options in childbirth. In their Executive Summary of The Nature and Management of Labor Pain, they shared that 99% of United Kingdom maternity units responding to a national survey said that nitrous was available to laboring women during childbirth. Additionally, in a national survey of women just after childbirth, 60% said they used the nitrous and, of those, 85% rated their pain relief with nitrous as “good” or “very good”. Around the same time, a US survey of pharmacological methods of pain relief did not even mention nitrous oxide. There were however, two forward-thinking (or should we say backward-thinking) hospitals that had already been using nitrous oxide – one of which, The University of California San Francisco, had been offering nitrous routinely for over 30 years!
While researching this topic, I was gob smacked to learn that the second hospital was the University of Washington because in the 11 years I practiced as a doula in Seattle, I had never seen or heard of nitrous being used there. So this might be a worthwhile moment to acknowledge that it was, in fact, my doula trainer, and long-time mentor/inspiration, DONA International, founder, and author, Penny Simkin, who suggested to the lead investigator of the review, Judith Rooks, CNM, that they include nitrous in their investigation of pain management in labor. You can read more about the systematic investigation in this Lamaze International/Science and Sensibility blog post interview with Rooks.
Later, in 2012, the Agency for HealthCare Research and Quality examined the use of nitrous oxide and compared it with other methods of pain management for intended vaginal deliveries. They determined there was very little quality data in the literature on the effectiveness of nitrous on pain management, however, satisfaction could be measured. What resulted was a thorough comparison. At that time, only 5 centers were using nitrous: UCSF and UW (as mentioned above), another hospital in Brewster, Washington, Vanderbilt Hospital in Nashville, and interestingly, St. Joseph Regional right here in Lewiston, Idaho! Finally, it was catching on and within the last 2 years, nitrous has become increasingly available as a pain relief option in US hospitals including here in the Treasure Valley.
A possible reason for the resurgence of interest in the pain relief method might also be the 2012 FDA approval of safety equipment to administer a 50% concentration of nitrous oxide with a 50% oxygen, as suggested by Catherine McGovern, RN who has written an article on the subject for DONA International’s December issue of International Doula. (available to members.)
For optimal delivery and safety, the laboring woman administers the inhaled medication herself by holding the mask over her mouth and nose. Self-administration allows the laboring woman to “time” her inhalation to her contractions and to coordinate the peak analgesic affect to about 60-90 seconds after inhalation. It also ensures safety and prevents the woman from inhaling too much nitrous which could result in her losing consciousness – a very rare occurrence since self-administration is required and a woman would become too drowsy to continue to hold the mask before she would become unconscious. For an expanded discussion on nitrous from Judith Rooks, see Our Bodies, Ourselves.
(It is important to know that this medication is defined and regulated as a prescription drug – which means doctors and midwives will need to “write for it”. Having a conversation with your care provider ahead of time to make sure that the option is a “standing order” for you is important in the moment you are trying to decide about pain management options.)

Lisa Arnold used nitrous at the birth of her daughter, Lilli in April of 2015 at St. Luke’s in downtown Boise. She described how it helped her during labor: “It was exactly what I needed during transition. I liked how I was able to use it when I felt I needed and also take a break from it at any time. Since the mask was not attached to me, it gave me the freedom to easily move from laying down to (sitting up on) the birth ball. Needing to the hold the mask and take deep breaths gave me something to concentrate on when the pain was very intense and its effects were mild and calming allowing me to feel in control and be present at such an amazing moment in our lives.”
While movement is possible using nitrous, it stands to reason that with drowsiness a predominant side-effect, any woman wanting to use nitrous in an upright position will need more careful observation, but I have personally had clients on birth balls, birth stools, and hands & knees positions while using the mask.

To ensure the fullest delivery of the medication, she should make sure the seal of the mask is tight on her face and inhale deeply. When done correctly, a low “rumbling” sound will be heard (and a vibration felt) from the nitrous tank and hose that carries the gas.
There has been some concern that nitrous poses an occupational risk for nurses, doctors and others in the birth room, (particularly those attempting to conceive or in their first trimester of pregnancy) but those concerns diminished with the FDA approved delivery system which includes a “scavenging system” that collects 70% of the exhaled nitrous. Laboring mothers are told to exhale back into the mask so that the majority of the exhaled gas is collected and deposited into a waste system through another hose.

What is Nitrous Oxide?
Nitrous Oxide is a naturally occurring* non-flammable, odorless and colorless gas that is quickly eliminated from the body through the lungs so it doesn’t accumulate in the mother’s body and has no adverse affects on the baby. *In nature it is produced by bacterial processes of biological decay. Man-made nitrous is usually the result of burning fossil fuels.
Safe for Mother and Baby
In the spring of 2014, I asked Nurse-Midwife, Kristi Rhodes to give a presentation on nitrous oxide- which had just been approved for use by Boise’s St. Luke’s Hospital – at our local conference for doulas. Kristi shared (with several references to Rooks who has likely written the most about its use in childbirth in the past 15 years) that no studies or observations have found any adverse affects on baby – no respiratory depression or increased need for neonatal resuscitation. Newborn responsiveness, alertness and early breastfeeding appears to be unaltered with the medication. In addition, there is no extra monitoring, so mothers can use the mask and still move into positions that provide comfort and progress as long as they are close to the nitrous tank.

In addition to showing no risks to baby, there appears to be little adverse outcomes for the laboring moms since the gas is eliminated through the lungs the effects are transient. Some women experience nausea and vomiting but since that is also common in the later part of labor, it is unclear if it is truly caused by the nitrous. More commonly, a woman might feel drowsy, or light-headed. The biggest complaints I have seen from my own clients have been ones that span the range of not liking the mask (but being quite satisfied with the relief they experienced – something like a relief of anxiety – knowing the physical sensations of the contractions are still there but caring little or far less) to being unhappy with the nitrous altogether because it didn’t stop the pain. In those cases, the fact that nitrous is eliminated so quickly from the body means there is no delay in moving on to an epidural if the client so chooses.
How does Nitrous Oxide Work?
While the definitive answer has yet to be confirmed, it appears that nitrous activates endogenous (naturally occurring) opiates such as endorphins (and likely dopamine) creating a euphoria (hence the name laughing gas) and/or modulating the perception of pain in the brain (hence many women’s ability to continue with labor when they felt they could not prior to inhaling the nitrous). Dr. William Camann, the immediate-Past President of the Society for Obstetric Anesthesia and Perinatology, described what women experience as “diminished pain, or a continued awareness of pain, without feeling bothered by it”.
Understanding how nitrous works will help tremendously in making an informed choice about when/how to use it and will likely play a factor in satisfaction with the pain management option.
Certified Nurse-Midwife, Georgianna Ainslie recently posted this article on her practice’s Facebook page. I asked her what she felt most people should know when they are considering using nitrous in labor.
“I think that one of the big points is to be clear about what you want an intervention to do because that will impact your results. If a woman is wanting all of the pain to go away, nitrous is not the answer, but if she is looking for something to help her get her focus back, help her relax and/or give her a little assistance to ‘get over the hump’ of transition, nitrous is a good solution. I also love that it is cheap, has no long-term impact, and has very minimal requirements as far as monitoring, etc. Nitrous, of itself, does not require an IV, or extra fetal monitoring (because it has no impact on the baby). We will want to monitor Mom’s oxygenation status with a pulse-oximeter for about 10 minutes, but then that is it. I love having more options for women!” ~ Nurse Midwife, Georgianna Ainslee

As a doula, I have seen nitrous work best toward the end of labor. Interestingly I have found that my clients who use nitrous before say 7-8 cm have chosen to get an epidural after trying the nitrous oxide. I am not sure if that is because change is not happening fast enough for them to remain with this “first level” pain reliever or because they somehow expected it to relieve more pain than it does. However, those who waited and used nitrous in transition, have made it to the end without an epidural. A few have asked for the epidural while they labored with the mask but by that point their labor progressed too fast to get the fluids in that they would have needed to start an epidural. While they waited for the bag of fluids to run, they ended up becoming complete and pushing, sometimes even moving beyond the need for the nitrous because they were now pushing – experiencing the contractions in a more active and tolerable way – that they chose to leave the mask off and simply push out their babies. While that might feel overwhelming in the moment, all those moms felt so pleased they did not get the epidural and happy that they had something that could take the edges off the pain enough to get them through it.
This is great option because it is important to note that nitrous has no effect on the labor itself making it a wonderful option for many women. With epidural, there is always the risk of the adverse effects such as lowered blood pressure, slowing contractions, lengthened pushing phase, fever and perhaps a need for an assisted vaginal delivery (vacuum extractor or more rarely, forceps). Nitrous does not appear to affect contractions or to diminish the laboring woman’s own oxytocin.
Who Should Use Nitrous Oxide?
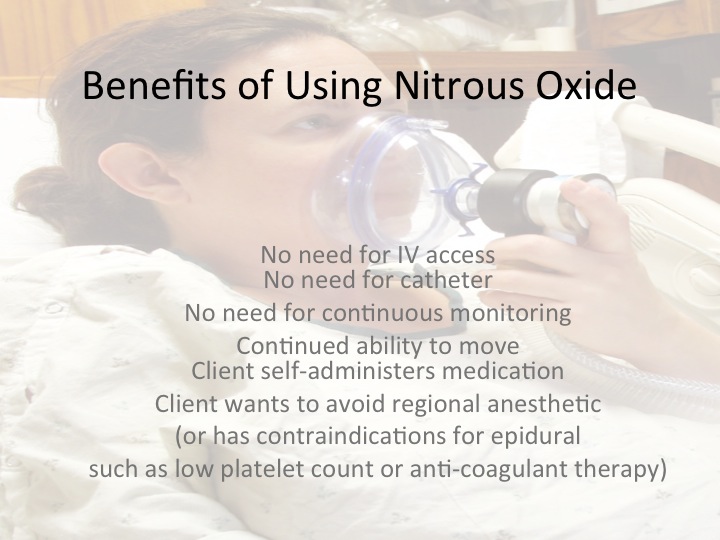
Because epidural comes with the need for IV medication and continuous fetal monitoring, nitrous, which has none of these requirements or risks, can be the perfect option for laboring mother who wants to avoid most interventions. It can also be excellent for a woman who cannot get an epidural due to a spinal injury or anomaly or whose platelets are so low she cannot get an epidural.
Nitrous is also incredibly beneficial for the woman who is experiencing significant anxiety. Heather Morgan had two out-of-hospital, unmedicated vaginal deliveries here in Idaho before moving out of state. Her first birth was unusually fast and her second, unusually long and hard. She gave birth to her third baby in Virginia, and was the first patient to use the nitrous oxide in the hospital she delivered in. She shared her experience with me:
“After having such a difficult labor with my second baby, I had a tremendous amount of anxiety and fear going into my third birth. I knew I didn’t want an epidural, but wasn’t willing to suffer the way I had with my last labor. Once I start transitioning, the fear kicked in which took my pain to a new level. I started to panic and told my husband I wanted an epidural. I was insistent. I absolutely didn’t want to go to “that place” ever again. As the anesthesiologist was discussing the risks of the epidural (and my mind was screaming: ‘don’t do this’), my midwife said, “How do you feel about nitrous?” I immediately replied “YES!” I had been reading about it and just hadn’t brought it up to her to see if it was an option. My baby came at 38 weeks so I thought we had time to discuss it. My body completely relaxed as I breathed it in and I could feel my baby coming down with every contraction. I wouldn’t say the pain was any better necessarily, but my body and MIND were able to let go completely, which is exactly what I needed. I went from 7cm to 10cm in 20 minutes. I felt no nausea from it, just relaxed and fearless. My midwife said she could see my muscles relax all over my body. I was so grateful there was a safe option for me and my baby. I needed healing from my previous birth and it was achieved largely because nitrous was an option for me.”
Who Should Not Use Nitrous?
Nitrous is not suitable (or usually necessary) when an epidural is in place or narcotic medications have been administered. Some contraindications do exist and all options should be discussed with care providers at the time of making an informed choice. A few known contraindications are: increased intracranial or intraocular pressure, bowel obstruction, pnuemothorax, emphysema, pulmonary hypertension and anyone with a current B12 deficiency and MTHFR gene mutation.
Where is Nitrous Available?
Here in Boise, we are lucky that both St. Luke’s and St. Alphonsus labor & delivery floors have nitrous oxide as an option for laboring women. St. Luke’s found the option to be so well-recieved that they have two machines available now and St. Alphonsus is quickly finding the same interest from laboring women. Of course, it will be used by more laboring mothers if their care providers discuss the option ahead of time. Nurse-Midwife, Amy English-Burt, with the St. Alphonsus Midwifery Group has also had wonderful experiences with her clients using nitrous oxide and shared her thoughts with me:
“It has proved helpful for so many situations and procedures including IV starts, exams, ECVs, labor, operative birth, and even laceration repair and postpartum procedures. It has quickly proven to be an asset for women who desire natural childbirth but struggle to remain focused. In short I love it!” ~ Nurse Midwife, Amy English-Burt
Here in Boise, nitrous oxide is also available out-of-hospital too. I first heard about nitrous in 2001 from a German midwife I worked with at Puget Sound Birth Center in Kirkland, WA and I understand that her midwifery practice is the first to use it out-of-hospital in Washington State. Here in Boise, nitrous oxide is available for labor at the free-standing birth center, Boise Women’s Health & Birth Center. Having nitrous oxide available in birth centers may prevent the need for transport to the hospital in some cases so it is wonderful that it is an option here for those who desire a home or birth center experience.
Other uses for Nitrous Oxide
There can be other times when asking for nitrous oxide would also be appropriate. It might be very appropriate for some people when having an IV hep/saline lock placed. In addition, nitrous can also be beneficial for use during an external version to turn a breech baby or, as Amy English-Burt mentioned above, it might be helpful after delivery as well.
From a doula’s perspective, I would add is this – if you choose to use nitrous and deliver your baby vaginally, you might consider the pros and cons of asking the nurses to keep the machine hooked up until after the delivery of your placenta and any possible repair you might need. While most women have no issues and do not need the nitrous at this point, I have seen a few instances where the option of the nitrous during these moments would have been very helpful and, in those cases, it had been broken down and removed from the room already.
So, even if you deliver with no pain medications at all, if your birthing facility has nitrous oxide, know that you may find it helpful outside of labor and delivery of your baby as well and if that is the case, don’t hesitate to ask for it!


Stacie
30.11.2015 at 10:27 pmI am glad this is becoming more available. I did know UCSF offered it. For me, nitrous actually makes me anxious, so I don’t think I would risk it in labor (that’s my dental experience with it — I had rising panic). Great post :).
Kyndal
30.11.2015 at 10:42 pmStacie, while some do experience more anxiousness, it is pretty rare. I wonder it it could be because the composition is higher at the dentist. Since it is 50/50 nitrous oxide and oxygen for birth, I think that may decrease that risk.